呼出气一氧化氮对于支气管哮喘诊治的价值
2016/07/07
费凡 黄茂
南京医科大学第一附属医院(江苏省人民医院) 210029
南京医科大学第一附属医院(江苏省人民医院) 210029
支气管哮喘(哮喘)是一种以慢性气道炎症为特征的异质性疾病,监测哮喘患者气道炎症的水平对于早期诊断及治疗后评估病情尤为重要。临床用于哮喘诊断与治疗的监测方法主要是根据临床症状、体征及肺功能检测等,而这些并不能直接反映气道炎症,且易受很多因素的影响。近年来研究发现,呼出气一氧化氮(FeNO)可较好的反映嗜酸粒细胞性炎症。本文将FeNO在哮喘诊治中的应用做一介绍。
一、FeNO的产生与测定
1. FeNO的产生
FeNO产生的主要机制是过敏性炎症刺激物诱导呼吸道上皮细胞产生一氧化氮合成酶(NOS)增多,经过一系列氧化还原反应产生过量的一氧化氮(NO)并可以通过呼出气测定。大量的实验证据表明,FeNO 测定可以作为一种非创伤性的方法直接量化气道炎症[1-2]。
2. FeNO的测定、参考值和影响因素
(1)测定:呼出气气流、软腭的低垂和死腔通气都会影响呼出气的NO水平。因此,呼出气NO通常实在对着一障碍物作单口呼气时测定,以防止混有鼻腔的NO成分,最通常的鼻气流中NO是使用化学发光仪从一侧鼻腔取气体样来测定。
(2)参考值:ATS建议将FeNO成人水平分为<25 ppb、25~50 ppb以及>50 ppb三组,儿童为<20 ppb、20~35 ppb以及>35 ppb三组[3]。其中成人<25 ppb,儿童<20 ppb,可初步排除嗜酸粒细胞性炎症,不建议给予糖皮质激素治疗;成人>50 ppb,儿童>35 ppb,提示嗜酸粒细胞性炎症可能,并建议有症状者应该给予糖皮质激素治疗;成人25~50 ppb,儿童20~35 ppb,应警惕并行进一步临床评估。另外,成人25~50 ppb时,考虑存在轻度的嗜酸粒细胞性炎症,此时应关注患者的临床症状、体征以及其他相关实验室参数;而成人>50 ppb时,也提示有过敏原暴露的风险[4]。
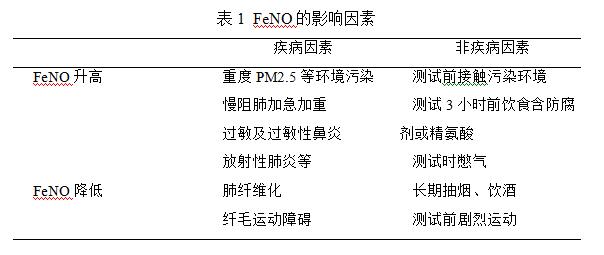
(3)影响因素:见表1。
二、FeNO在成人哮喘诊断中的价值
有典型症状和体征的哮喘患者,除外其他疾病引起的喘息、气急、胸闷和咳嗽后,可作出临床诊断;对不典型病例,应作支气管舒张或激发试验以及PEF变异率测定,阳性者可确诊。支气管激发试验反映气道高反应性(AHR),但存在操作复杂、需耍专门的仪器、费时等缺点,且有诱发支气管痉孪的风险。而FeNO操作简单,安全可行,研究表明在对哮喘的诊断上有着不低于支气管激发试验的价值。Berkman[5]等在一项 85例哮喘疑似病例的研究中发现,FeNO 诊断哮喘的敏感性是82.5%,特异性是88.9%;而同时应用乙酰胆碱行支气管激发试验诊断哮喘的敏感性和特异性则分别为87.5%和 86.7%,两者差异不明显,提示FeNO可用于哮喘的诊断。Smith[6]等研究发现,FeNO检测联合支气管激发及舒张试验后,其敏感性及特异性可提升至94% 和93% 。
此外,有研究[7]应用ROC曲线对FeNO诊断支气管哮喘的准确性进行判定,表明FeNO诊断支气管哮喘的最佳临界值 为53.25ppb,灵敏度为87%,特异度为70%,曲线下面积为0.882,95%可信区间为(0.814,0.949),此时FeNO诊断支气管哮喘准确性较高。Pedrosa M等[8]研究了114名具有持续哮喘症状的成人患者,并且伴有正常的肺功能以及支气管舒张试验阴性,研究发现,当FeNO的截点是40 ppb时,诊断成人哮喘的敏感性74%,特异性72.5%。因FeNO与嗜酸粒细胞性气道炎症相关,可适用于过敏性哮喘的诊断;非嗜酸性细胞炎症优势型哮喘时FeNO不高,此时诊断应慎重。
三、FeNO在哮喘治疗方面的应用进展
1.对于糖皮质激素(激素)治疗敏感性的预测
激素是哮喘治疗的一线用药,有研究表明,FeNO可以用来预测哮喘对于激素的反应,激素治疗后FeNO 高的患者比FeNO低的患者肺功能及控制评分的改善更加显著。Warke[9]等的研究 结果显示 FeNO与痰诱导嗜酸粒细胞计数的有显著相关性 (r=0.78,P<0.001)。Schleich等[10]对295例哮喘患者的系统回顾性研究表明,FeNO检测≥41 ppb时患者诱导痰嗜酸粒细胞计数≥3%(敏感性65%、特异性79%)。还有报道显示FeNO和痰诱导痰嗜酸粒细胞计数[11-12]、血嗜酸粒细胞计数[13-15]、血清嗜酸粒细胞阳离子蛋白[16-18]以及血清IgE[19-21]水平相关。2011年ATS关于FeNO临床应用指南指出,FeNO≥50 ppb提示存在明显的嗜酸粒细胞性气道炎症,激素治疗敏感性较高;而FeNO≤25 ppb时,嗜酸粒细胞性气道炎症可能性很小,提示对激素敏感性不佳,不推荐激素治疗。Taylor[22]发现,与PEF、肺功能以及支气管舒张试验比较,FeNO对预测激素敏感性有更高的价值;对于激素治疗不敏感的哮喘患者的FeNO值大多(91-95%)介于20-30 ppb;而哮喘患者激素敏感性较高时的FeNO值大多(79-82%)是≥47 ppb。
2.对于哮喘治疗方案调整的指导
目前哮喘临床治疗,主要是根据患者临床症状的控制情况进行降阶梯治疗,但仅仅根据哮喘的临床控制症状准确性不强,临床医生往往会被症状控制干扰,影响其对于哮喘控制的正确把握。指南中早就提及FeNO对于激素治疗方案调整有指导意义,但如何根据FeNO进行调整,目前并未有定论。Powell[23]等将220位哮喘孕妇随机分为基于症状的控制组和基于FeNO的FeNO组,FeNO和控制组在哮喘加重比例差异明显(FeNO组加重比0.288 vs 控制组 0.615,p = 0.001)。数个研究亦表明[24-26],将FeNO联合症状控制组的恶化数量要低于仅仅基于症状控制组。James F等人[27]亦发现,对比现行的症状评估,FeNO联合症状控制的评估对病人更有益,FeNO在成人哮喘的评估和管理中有着重要的作用。上述文献报道中,基本上将哮喘患者加重的次数作为评估病情恶化的程度,但是这种方法没有考虑到患者可能存在多种恶化的方式,因此有人考虑用距离第一次病情加重的时间或者病情加重的速度来评估病情。Shaw[28]和Smith[29]等用病情加重的速度作为评价指标并进行荟萃分析,结果发现基于FeNO的治疗组病情恶化速度显著降低;此外,与对照哮喘管理策略相比,基于FeNO的哮喘管理策略恶化的速率较降低超过40%。
在哮喘患者(儿童和成人)使用的所有治疗或治疗方法中,效益比是很重要的一个考虑因素。大多数文献报道结果均显示,基于FeNO的哮喘管理策略和基于临床症状管理策略相比,在实验结束时激素使用的总量相似或者更低。Persijn J等[30]进行了一项有211参与者的临床研究,将FeNO和症状评分一起作为临床用药的基准,对比与目前仅仅以症状控制作为依据的治疗方法,在激素用量和花费上更有优势(p = 0.003)。然而在Szefler[31]的研究中,结果却恰恰相反。究其原因,发现受试者有高水平的哮喘控制。此外,FeNO水平高时,尽管哮喘控制可,也需增加ICS的剂量;但是当FeNO水平低,除非所有其他哮喘参数也被控制,否则ICS剂量不能被减少。因此,ICS剂量在FENO组更高并不奇怪。在比较FeNO水平的哮喘的管理策略和一般临床管理,目前的研究普遍表示,基于FeNO的管理的效益比和病情恶化速度更具有优势,并且FeNO水平测试在成人哮喘的评估和管理具有重要作用,进一步的研究将有助于评估成人哮喘FeNO水平测试的确切作用。
四、总结
FeNO检测无创、简单,对于提示Th2型气道炎症的激素反应性可靠性较高,在哮喘的评估和管理中有着重要的作用。FeNO 作为诊断哮喘的辅助手段,能够协助临床医生诊断嗜酸性粒细胞性哮喘。其对于激素敏感性的预测能够帮助临床医生有效筛选出患者并决定哮喘治疗的策略,例如是否调整激素治疗剂量。基于FeNO的临床用药管理比现行的症状控制管理在平均恶化速度以及效益比中都显示出了明显差异。总之,FeNO在嗜酸性粒细胞性哮喘的初筛、鉴别诊断、治疗评估、用药调整等应用中均具有较大的临床价值,并且对于哮喘的预后有着积极作用,但还需要进一步研究来证实。
参考文献:
1. Kharitonov SA, Chung KF, Evans D, et al. Increased exhaled nitric oxide in asthma is mainly derived from the lower respiratory tract[J]. Am J Respir Crit Care Med. 1996, 153(6 Pt 1): 1773-1780.
2.Jatakanon A, Lim S, Kharitonov SA, et al. Correlation between exhaled nitric oxide, sputum eosinophils, and methacholine responsiveness in patients with mild asthma[J]. Thorax, 1998, 53(2): 91-95.
3.Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels(FeNO)for clinical applications[J]. Am J Respir Crit Care Med, 2011, 184(5): 602-615.
4. Spitale N, Popat N, McIvor A. Update on exhaled nitric oxide in pulmonary disease[J]. Expert Rev Respir Med, 2012, 6(1): 105-115.
5. Berkman N,Avital A,Breuer R et al.Exhaled nitric oxide in the diagnosis of asthma: comparison with bronchial provocation tests.[J].Thorax: The Journal of the British Thoracic Society,2005,60(5):383-388.
6. Smith AD;Cowan JO;Brassett KP.Use of exhaled nitric oxide measurements to guide treatment in chronic asthma[J].New England Journal of Medicine,2005,352:2163-2173.DOI:10.1056/NEJMoa043596.
7. Dupont LJ, Demedts MG, Verleden GM. Prospective evaluation of the validity of exhaled nitric oxide for the diagnosis of asthma[J]. Chest, 2003, 123(3): 751-756.
8. Pedrosa M, Cancelliere N, Barranco P, et al. Usefulness of exhaled nitric oxide for Questionnaire.Respir Med, 99 (2005)[j], pp. 553–558.
9. Warke TJ,Fitch PS,Brown V,et a1.Exhaled nitric oxide correlates with airway eosinophils in childhood asthma[J]. Thorax,2002,57:383 387.
10. Schleich FN,Seidel I。,Sele J,et a1.Exhaled nitric oxide thresholds associated with a sputum eosinophil count≥3% in a cohort of unselected patients with asthma[J].Thorax, 2010,65:1039-1044.
11. M.A. Berry, D.E. Shaw, R.H. Green, C.E. Brightling, A.J. Wardlaw, I.D. Pavord.The use of exhaled nitric oxide concentration to identify eosinophilic airway inflammation: an observational study in adults with asthma[J]Clin Exp Allergy, 35 (2005), pp. 1175–1179.
12. S.J. Szefler, H. Mitchell, C.A. Sorkness, et al.Management of asthma based on exhaled nitric oxide in addition to guideline-based treatment for inner-city adolescents and young adults: a randomized controlled trial.Lancet, 372 (2008), pp. 1065–1072
13. Y. Sivan, T. Gadish, E. Fireman, R. Soferman.The use of exhaled nitric oxide in the diagnosis of asthma in school children[J]J Pediatr, 155 (2009), pp. 211–216.
14. A. Fuhlbrigge, D. Peden, A.J. Apter, et al.Asthma outcomes: exacerbations.J Allergy Clin Immunol, 129 (2012), pp. S34–S48
15. S.L. Jones, J. Kittelson, J.O. Cowan, et al.The predictive value of exhaled nitric oxide measurements in assessing changes in asthma control.Am J Respir Crit Care Med, 164 (2001), pp. 738–743
16. Z. Zietkowski, A. Bodzenta-Lukaszyk, M.M. Tomasiak, R. Skiepko, M. Szmitkowski.Comparison of exhaled nitric oxide measurement with conventional tests in steroid-naïve asthma patients[J]J Investig Allergol Clin Immunol, 16 (2006), pp. 239–246.
17. J.D. Leuppi, C.M. Salome, C.R. Jenkinds, et al.Predictive markers of asthma exacerbation during stepwise dose reduction of inhaled corticosteroids.Am J Respir Crit Care Med, 163 (2001), pp. 406–412
18. C. Delgado-Corcoran, N. Kissoon, S.P. Murphy, L.J. Duckworth.Exhaled nitric oxide reflects asthma severity and asthma control.Pediatr Crit Care Med, 5 (2004), pp. 48–52
19. D. Cordeiro, A. Rudolphus, E. Snoey, G.-J. Braunstahl.Utility of nitric oxide for the diagnosis of asthma in an allergy clinic population[J]Allergy Asthma Proc, 32 (2011), pp. 119–126.
20. R.S. Zeiger, M. Schatz, F. Zhang, et al.Elevated exhaled nitric oxide is a clinical indicator of future uncontrolled asthma in asthmatic patients on inhaled corticosteroids.J Allergy Clin Immunol, 128 (2011), pp. 412–414
21. W.J. Calhoun, B.T. Ameredes, T.S. King, et al.Comparison of physician-, biomarker-, and symptom-based strategies for adjustment of inhaled corticosteroid therapy in adults with asthma: the BASALT randomized controlled trial.JAMA, 308 (2012), pp. 987–997
22. D.R. Taylor.Advances in the clinical applications of exhaled nitric oxide measurements[J].J Breath Res, 6 (2012), pp. 1–8.
23. H. Powell, V.E. Murphy, D.R. Taylor, et al.Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double-blind, randomized controlled trial.Lancet[J], 378 (2011), pp. 983–990.
24.H.L. Petsky, C.J. Cates, A. Li, J.A. Lynaston, C. Turner, A.B. Chang.Tailored interventions based on exhaled nitric oxide versus clinical symptoms for asthma in children and adults .Cochrane Database Syst Rev[J], 2 (2009), p. CD006340.
25. M.G. Cochrane, M.V. Bala, K.E. Downs, J. Mauskopf, R.H. Ben-Joseph.Inhaled corticosteroids for asthma therapy.Chest, 117 (2000), pp. 542–550
26. J.B. Soriano, K.J. Davis, B. Coleman, G. Visick, D. Mannino, N.B. Pride.The proportional Venn diagram of obstructive lung disease: two approximations from the United States and the United Kingdom.Chest, 124 (2003), pp. 474–481
27. James F. Donohue,Neal Jainb. Exhaled nitric oxide to predict corticosteroid responsiveness and reduce asthma exacerbation rates. Respiratory Medicine[J].Volume 107, Issue 7, July 2013, Pages 943–952.
28. H. Powell, V.E. Murphy, D.R. Taylor, et al.Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double-blind, randomized controlled trial[j]Lancet, 378 (2011), pp. 983–990.
29. A.D. Smith, J.O. Cowan, K.P. Brassett, G.P. Herbison, D.R. Taylor.Use of exhaled nitric oxide measurements to guide treatment in chronic asthma[J]N Engl J Med, 352 (2005), pp. 2163–2173.
30. Persijn J. Honkoop, Symptom- and fraction of exhaled nitric oxide–driven strategies for asthma control: A cluster-randomized trial in primary care. Journal of Allergy and Clinical Immunology[J].Volume 135, Issue 3, March 2015, Pages 682–688.e11.
31. S.J. Szefler, H. Mitchell, C.A. Sorkness, et al.Management of asthma based on exhaled nitric oxide in addition to guideline-based treatment for inner-city adolescents and young adults: a randomized controlled trial.Lancet[j], 372 (2008), pp. 1065–1072.
上一篇:
骨膜蛋白在支气管哮喘诊治中的作用
下一篇:
抗IgE治疗过敏性哮喘的长期有效性、安全性和成本效益分析









